
Healthcare in the United States spends somewhere between $285 billion and $570 billion a year on administrative costs that don’t contribute to patient outcomes. Even at the lower end, that’s twice what the country spends on cardiovascular care, and three times what it spends on cancer treatment.
Most of that spending isn’t fraud, or waste in the traditional sense. It’s skilled, well-intentioned people manually moving information from one place to another – reading a fax, retyping a referral, entering a home visit note into a system that didn’t receive it directly.
The technology to automate most of that work exists and has for some time. The gap, for most organizations, is that it hasn’t been built into the workflows where the cost is actually occurring.
Paper is still everywhere
Despite decades of digitization, paper hasn’t left healthcare – and the documents that still arrive by fax, by hand, and in payer-specific formats that share no common standard all contain information that needs to get into a system. In most organizations, a staff member is doing that manually, one document at a time.
Traditional OCR reads text from a document and outputs it. That’s one layer – but for most of the documents healthcare organizations actually deal with, it’s not enough. A printed, consistently formatted form is the easy case. The referral that arrives as a handwritten fax, the home visit note photographed in the field – traditional OCR either misreads these or fails on them entirely.
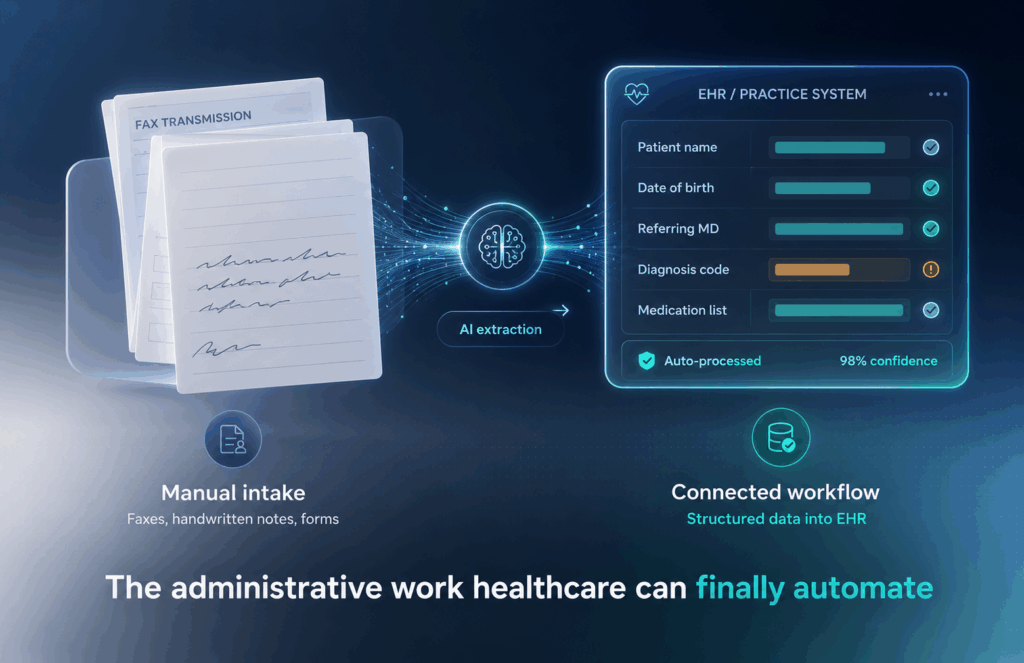
AI-assisted document processing handles that broader category: it reads handwritten content, interprets non-standard layouts, and extracts structured data from documents with no predictable field order. But the more significant capability is what can happen after the extraction. A confidence score is assigned to each field, and that score determines what happens next: high-confidence reads are passed downstream automatically; low-confidence reads are held for human review before they go anywhere. In a clinical environment, where a misread medication name or a transposed date has real consequences, that threshold is what makes the automation trustworthy enough to actually deploy.
Where it makes the most difference
Referral management. Referrals arrive as multi-page faxes with inconsistent formatting, handwritten additions, clinical notes from the referring provider mixed in with demographic fields. Someone has to read each one, determine whether the information is complete, and key it into the practice management or EHR system. When volume is high and staff bandwidth isn’t, referrals sit, some get missed, and there’s room for error at every manual step.
The full picture of what a well-built system looks like: a handwritten, unstructured fax arrives, the relevant data is extracted and structured, and if the confidence score clears the threshold, that record is pushed directly into the EHR or practice management system for appointment scheduling.
Home care documentation. Home health and hospice organizations manage a constant flow of paper – physician orders, medication lists from discharge packets, handwritten visit notes from the field. Without automation, each document requires manual transcription before it can support scheduling, billing, or care planning. With document processing built into the platform, intake data flows directly into clinical and operational systems from the point of capture, and the downstream workflows – care planning, billing, scheduling – start from complete information rather than waiting on a transcription queue.
Reimbursements and billing. When remittance documents arrive from payers, the system extracts claim data, maps it to the patient record, and flags discrepancies before they become denials. What previously required a billing specialist to manually review and enter moves through the workflow automatically, with human review reserved for the exceptions that actually need it.
Why the OCR layer is only part of the answer
There are SaaS products that handle OCR and confidence scoring, and they do that job well. But treating document extraction as a standalone problem misses where the operational value actually lives. Extracted data needs to go somewhere – into the EHR, the practice management system, the scheduling workflow – and how it gets there, in what format, through which integration, matters as much as how accurately it was read.
The organizations that get the most out of this investment are the ones that treat document processing as one layer in a connected workflow rather than a product to deploy in isolation. That means the confidence scoring isn’t just flagging fields for review – it’s determining which records move automatically into connected systems and which ones wait. It means the EHR and practice management integrations are built around how the organization actually uses those systems, not around a generic API handoff. And it means the existing stack stays intact – the goal isn’t to replace the tools that are working, but to make sure everything connects in the places where it currently doesn’t.
The practical question
Before the next contract renewal for a platform your team is working around, or the next budget conversation about administrative staffing, the question worth asking is this: how much of the manual work your team does every day could be automated – not with a new SaaS subscription, but built into the systems you’re already running?
MWE has been building custom healthcare software since 2003. We integrate AI-assisted document processing and workflow automation into existing healthcare platforms and build new ones where the right solution doesn’t exist yet. If you want to look at where the friction is in your workflows, we’re happy to start there →